Zits. Some people (wisely) are capable of simply letting them be, while others, such as myself and the folks on r/popping, struggle to avoid messing with them at every opportunity. I was watching Dr. Sandra Lee aka Dr. Pimple Popper when she was only a YouTube channel: squeezing out every last bit of pus is incredibly satisfying, all the more so when it is actually clinically indicated instead of making things worse. The process featured in a lot of Dr. Lee’s videos is called an “incision and drainage” (I&D), a procedure in which the doctor cuts the offending area open, cleans everything out, and preps the area for healing with packing and/or sutures.
Perhaps the queen mother of all zits is the pilonidal cyst, a collection of debris at the top of the buttocks that turns into an incredibly painful local infection. Due to the location, pilonidal cysts are capable of other horrifying things like forming connection channels into the rectum. If it’s that bad, Surgery gets involved, but up until that point…it’s the ED.
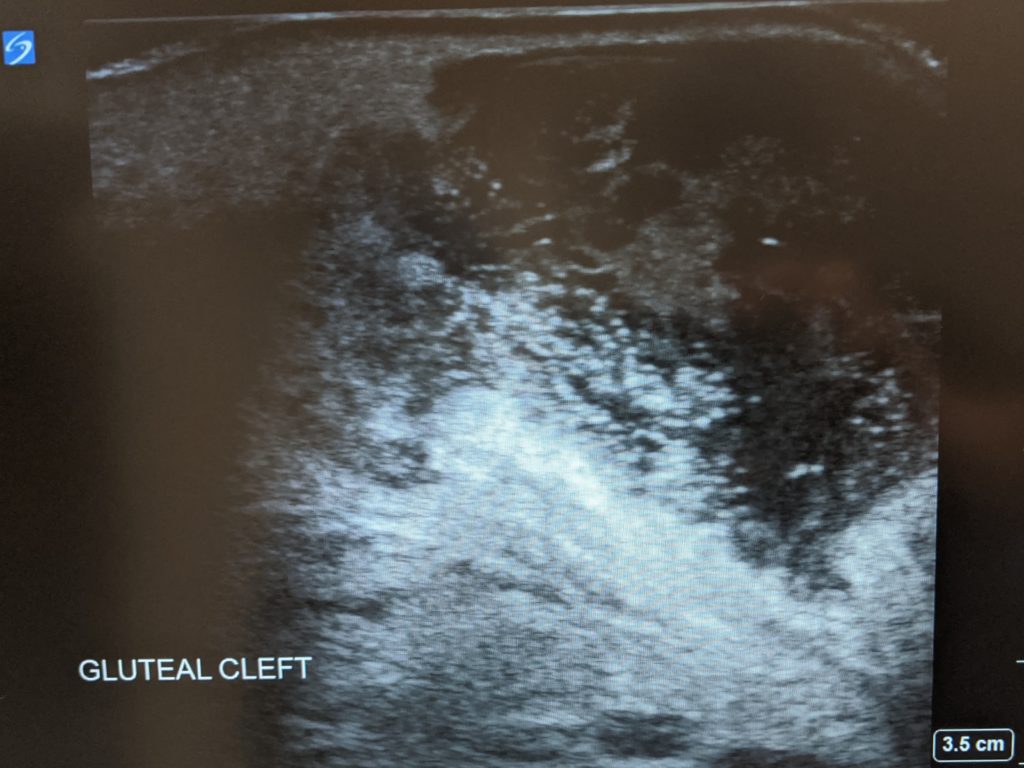
I have wanted to I&D a pilonidal cyst since I started residency. It’s one of ultimate popping experiences, but as I am going into Neurology, it’s not a procedure I’ll be doing after I move on from my General Pediatrics years. On my penultimate ED shift, it arrived. Enormous, painful, and ready to burst—so ready, in fact, it started leaking while we did the ultrasound, which revealed that it was just shy of a golf ball in size and depth. I could hardly contain my excitement. My attending was not amused, having already done this far too many times despite her young career. After prepping the site and anesthetizing the area, I went for it with an 11 blade while she stood ready with piles of gauze.
It was every bit as revolting as I had imagined. Brown, bloody pus launched from the cyst, traveling about half a meter toward the patient’s knees. Quick to react, my attending slammed a handful of gauze against the incision to prevent further spray. Her flashing eyes repeated the warning she’d given me outside the room against hitting her with ooze. I took the now-saturated gauze and replaced it with a fresh stack, expressing more thick liquid. My body issued warning gags, protesting against the putrid odor seeping through my surgical mask.
We pressed, soaked through gauze, and pressed some more, carefully draining a never-ending supply of foul alluvium for what felt like ages. When it finally ran dry, I flushed the cavity with a copious amount of sterile saline. A hole that deep can’t be sutured closed from the outside: it needs to heal from the inside out. To facilitate this, we packed the area, feeding an iodine-treated snake of gauze into the incision until it could hold no more, covering everything with a bandage.
I surveyed the scene. Although my person—and, more importantly, my attending’s—had been spared, the sheets, the hospital gown, and bed were not so fortunate. I disposed of stinking gauze by the armload before returning to the workroom to write my procedure note. “Pilonidal cyst,” I selected from the options. My attending glowered. I beamed.